AUCTORES
Globalize your Research

SHORT REPORT | DOI: https://doi.org/10.31579/2578-8949/025
*Corresponding Author: Cristina Martínez-Morán, Servicio de Dermatología. Hospital Universitario de Fuenlabrada. Madrid, Spain
Citation: Cristina Martínez-Morán, Begoña Echeverría-García1, Susana Córdoba, Jesús Borbujo, 2018, 10 Frequent Diagnosis in Dermatology. J .Dermatology and Dermatitis, DOI:10.31579/2578-8949/025
Copyright: © 2018 Cristina Martínez-Morán, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 08 March 2018 | Accepted: 09 May 2018 | Published: 23 May 2018
Keywords: Acne; fibroepithelial polyps; atopic dermatitis; seborrheic dermatitis; molluscum contagiosum; melanocytic nevi; psoriasis, actinic keratosis; seborrheic keratosis; viral warts
We present the more relevant aspects of the 10 most frequent dermatologic diagnostics: acne, fibroepithelial polyps, atopic dermatitis, seborrheic dermatitis, molluscum contagiosum, melanocytic nevi, psoriasis, actinic keratosis, seborrheic keratosis and viral warts. We describe their pathogenesis, clinical features, their management and preventive actions to avoid the progression of the conditions.
Dermatology is a challenging medical specialty which requires expertise in the treatment and the management of children and adults with skin disease. There are more than 4000 possible diagnoses and these involve conditions affecting the skin and appendages in every part of the body: the hair on the scalp and everywhere in the body, the nails and the mucosal lesions affecting the mouth and genital regions.
There are no consensus of the more frequent conditions diagnosed in a dermatology consultation, so it depends on the country, the ambiental factors such as latitude, altitude, population’s sun exposure, if the analyzed people worked outside or inside, etc…
As previously described in our report [1] of the outpatient activity in the dermatology department over the 2009 and 2010 years, the more frequent diagnosis were psoriasis, melanocytic nevi, eczemas (being atopic and seborrheic ezcemas the most frequent inside this group), seborrheic keratosis, actinic keratosis and viral warts. The next diagnoses in frequency were “other benign tumours” and “other cysts”, acrochordons and molluscum contagiosum. Being our purpose to choose the 10 more frequent diagnoses in dermatology to write the article for the Spanish journal of general practitioners [2] we preferred to include acrochordons and molluscum contagiosum better than epidermal cyst which may be included in the acne chapter.
Concept:
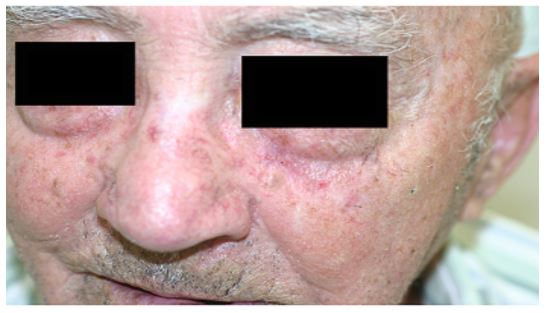
Acne vulgaris is a chronic inflammatory cutaneous disease of the pilosebaceous unit and the most common cutaneous disorder affecting adolescents and young adults. It has a significant impact in psychological morbidity with even suicidal tendencies [3, 4]. The prevalence of acne vulgaris in adolescents range from 35 to over 90 percent [5, 6].
In the pathogenesis of acne we must consider four pathogenic factors: follicular hyperkeratinisation (augmented corneocyte cohesiveness and proliferation), increased sebum production, Propionibacterium acnes (also known as Cutibacterium acnes) within the follicle and inflammation.
Papules, pustules, open and closed comedos, cysts, nodules and scars could be present in the same patient (Fig1), and description of lesions may be useful in the classification of the type and severity of acne and the patient’s management.

Differential diagnosis: it should be done with acneiform reactions, rosacea, drug-induced acne and perioral dermatitis.
Treatment: Predominant lesions and specific clinical features may determine the best approach. Topical therapies are preferred for mild forms of acne vulgaris. Topical retinoids may be beneficial in both inflammatory and comedonal acne. Topical antibiotics may be used in combination in order to reduce bacterial resistances. Systemic treatment is indicated in moderate to severe forms of acne. Isotretinoin in monotherapy, oral antibiotics such as tetracycline, which is widely used, and hormonal therapies, both combined or not with topical treatments.
Prevention and how to control the progression of acne: Because acne is a multifactorial condition, there are no significant strategies to prevent its development. Once the disease is established, using oil free cosmetics, and non-occlusive make up, is necessary to control acne, but medical strategies mentioned above are mandatory to treat this disease.
Concept: Acrochordons or skin tags are the most frequent mesenchymal tumours of the skin.
Clinical manifestations: Acrochordons use to be multiple pedunculated, furrowed or filiform lesions, skin coloured or darker (Fig2), and typical areas of involvement are skin folds like axilla, groin (Fig3), beneath the breast and in the neck or eyelids [7].


Differential diagnosis includes multiple benign cutaneous lesions: seborrheic keratosis, intradermal nevus; infectious diseases like viral warts and malignant tumours. In those cases, non ablational techniques are preferred to remove the lesions in order to make a histopathological analysis.Skin tags appears in the perianal area in Crohn’s disease, and when they coexist with fibrofolliculomas and trichodiscomas, a Birt-Hogg- Dubé syndrome must be suspected.
Treatment: It is not necessary because they are benign lesions, but curettage, electrocoagulation and cryotherapy can be performed. Electrocoagulation is our preferred technique.
Prevention and how to control the progression of acrochordons: No prevention for these skin tags has been described.
Concept:
Actinic keratosis (AK) also known as solar keratosis is a cutaneous lesion that results from the proliferation of atypical epidermal keratinocytes. AKs represent early lesions on a continuum with squamous cell carcinoma (SCC) and occasionally progress to SCC [2, 8]. AKs are among the most common reasons for visits to dermatologists and they are increasing its incidence with the population ageing.
The main cause of AK is exposure to ultraviolet radiation (UVR). However, cutaneous Human Papilomavirus may act as a co-carcinogen with UVR. Actually, prevalence and viral load is significantly higher in actinic keratosis than in SCC, suggesting that the virus may play a role in the early stages of carcinogenesis [9]. In an interesting study Padilla et al. showed the different genes expression profile in normal skin, AKs and SCC, revealing in AK and SCC a similar up-regulation of genes, down-regulated in normal skin and a similar down- regulation of genes upregulated in normal skin, confirming the common origin of both lesion and in particular AK as a precursor lesion of SCC [10].
Clinical manifestations: AKs often present as solitary or multiple erythematous and scaly macules or papules(Fig4), most commonly detected in adults with fair and chronic sun exposure and damaged skin.
AKs are generally asymptomatic, but some patients experience local tenderness or a stinging sensation.Diagnosis and differential diagnosis: AK is frequently diagnosed clinically through a combination of touch and visual inspection combined with dermoscopy [11]. They use to be more easily identified through the detection of rough texture. Differential diagnosis SCC, benign lichenoid keratosis, superficial basal cell carcinoma, inflamed seborrheic keratosis, porokeratosis and inflammatory dermatoses such as psoriasis.
Treatment: Treatment options [12] for AK include destructive therapies (eg, surgery, cryotherapy, dermabrasion, photodynamic therapy [PDT]), topical medications 5-fluorouracil, imiquimod, ingenol mebutate, diclofenac, and chemical peels such as trichloroacetic acid. In general, lesion-directed treatments, such as cryotherapy and surgical procedures, are the primary approach for isolated lesions. Field-directed therapies, such as topical 5-FU, imiquimod, ingenol mebutate, and diclofenac, are particularly useful for treating areas with multiple AKs [13].
In isolated lesions, we prefer criotherapy, but in field cancerization, we choose photodynamic therapy with BF-200 ALA or topical 5-fluorouracil.
Prevention and how to control the progression of AKs: Close surveillance of elderly people with severe photodamage is extremely recommended for prompt diagnosis. Because AKs appears over damaged sun skin areas, photoprotection since childhood is mandatory to minimize progression and to prevent the condition.
Concept:
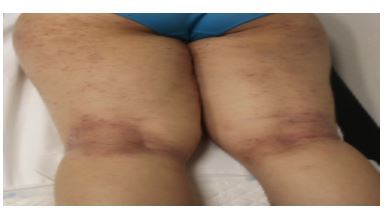
Atopic dermatitis (AD) is a chronic pruritic inflammatory skin disease most frequently affecting children, but also in adults, often associated with elevated serum level of immunoglobulin E and a personal or family history of atopy (eczema, asthma, and allergic rhinitis). AD is the most frequent eczematous eruption in pediatric age [2].
Clinical manifestations: Dry skin and severe pruritus are the cardinal signs of AD and this one impacts in the quality of life. Erythematous, scaly and lichenified plaques over the extensor surfaces of the extremities are often present (Fig 5).
However, the clinical presentation is highly variable, depending upon the patient's age and disease activity (table 1).
| Clinical lesions according to age | |||
Lactants | Children | Adults | ||
Age | Zero to two years | Two to sixteen years | From puberty | |
Morphology | Acute ezcema: erythema, fisures and cracks | Xerosis, excoriations, lichenified plaques | Lesions localized and lichenified | |
Location | Scalp, cheeks, face, extremities extensor surfaces | Flexor extremities surfaces, retroauricular area and eyelids | Neck, wrists and dorsum of feet | |
Table 1. Clinical aspects in atopic dermatitis according to patient’s age.
Differential diagnosis: Allergic or irritant contact dermatitis, seborrheic dermatitis, psoriasis and scabies.
Treatment: The goals for atopic dermatitis are to reduce symptoms (pruritus and dermatitis), prevent exacerbations, and minimize therapeutic risks. Topical corticosteroids or topical calcineurin inhibitors and emollients are the basis of the treatment in AD. Pruritus can also be treated with antihistamines. Phototherapy or systemic immunosuppressant treatment may be necessary to achieve adequate disease control in moderate to severe cases. Hospitalization is a good treatment option in severe atopic dermatitis with bad ambulatory control. We use to hospitalize patients with severe AD when other strategies have failed, we treat them only with topical care and in a week period, they improve significantly. New biological therapies are now being studied and we hope that they achieve better control of the disease, as well as biologics have get it in psoriasis.
Prevention and how to control the progression of AD: emollients, syndet products and not using hot water that produces dry skin are habitual recommendations in patients with atopic dermatitis, but in severe cases, those actions use to be ineffective.
Concept: Melanocytic nevi are abnormal benign proliferations of melanocytes in the skin that histopathologically demonstrate the formation of nests of cells. They may be present at birth or may appear at any time (congenital vs acquired melanocytic nevi).
Pathogenesis: The presence of multiple nevi comes from the result of a genetic predisposition (presence of isolated polimorfisms in nucleotids, germ line mutations in NRAS o BRAF…) and climatic conditions such as extensive solar exposure (which has been associated with larger and atypical nevi), chronic sun exposure in mediterranean countries (which has been associated with multiple small nevi without clinical atypia) andlatitudes close to the equator. All these are the reasons why primary prevention is so important. We must inform the patient about the nocive effects of intense and chronic sun exposure, focusing on the early childhood [14,18].
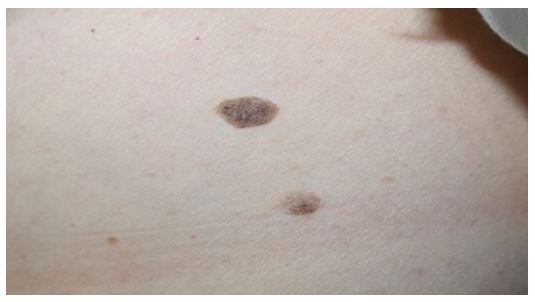
Es por esto por lo que la prevención primaria es fundamental, informando al paciente de los efectos nocivos de la exposición solar tanto crónica como intensa insistiendo principalmente en las edades tempranas de la vida [14].Congenital nevi are present in the first 6 months of life and 1 percent of the newborns present them. Clinical manifestations: congenital nevi (Fig6)

use to be asymptomatic and larger than acquired nevi (Fig7), but there is tremendous variability in the size of the individual lesions. Nevi can appear in the skin and mucous membranes. A patient with multiple nevi needs to be carefully inspected in order to find suspicious lesions and to biopsy them if necessary.

Diagnosis and differential diagnosis: to differentiate acquired nevi from melanoma, clinical examination, anamnesis and dermoscopic features are required. The ABCDE rule [19,20] encompasses several clinical features of melanoma including Asymmetry, Border irregularity, Colour more than 3 in the same lesion or variation, Diameter greater than 5 mm and Evolving (a new or changing) lesion.
Treatment: Melanocytic nevi are benign lesions and most of them require no treatment. Surgical excision for biopsy is recommended in doubtful lesions and changing nevi. Other excision indications could be traumatic lesions located in skin folds or in rubbing with clothes. Tangential excision is not recommended.
Prevention and how to control the progression of melanocytic nevi: Photoprotection from the early childhood avoiding sun exposure, and sunburn, observation and autoexploring melanocytic nevi are best strategies to reduce the risk of developing malignant melanoma from a melanocytic nevi or the novo.
Concept and clinical manifestations:
Molluscum contagiosum are caused by a Poxvirus. They can occur as solitary or multiple dome-shaped, umbilicated papules, 2-8 mm in diameter, whitish or yellowish, with predilection for flexural areas, the head and neck and genitalia in children and adolescents (Fig8). Sexual and fomite transmission may occur. Extensive lesions can occur in immunocomprised patients and atopic children [21].

Differential diagnosis: adnexal tumours and basal cell carcinomas especially in solitary and big lesions.
Treatment: Spontaneous regression often occurs, so treatment should be conservative and always agreed upon parents which need to know treatment options and that no treatment is one of them. Multiple therapies can be used if needed but curettage is the preferred one [2,22].
Prevention and how to control the progression of molluscum contagiosum: in atopic patients, treating eczema may improve the control of the disease and the spreading of molluscum. Avoiding direct contact between infected and theoretical non-infected children might be a good choice. However, this measure will mostly fail due to the lack of knowledge about the incubation period and about how long needs the skin to eliminate the virus once clinical lesions are removed.
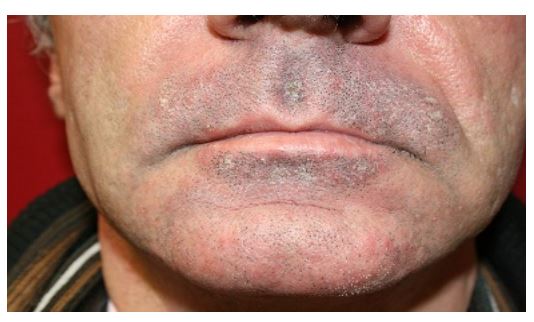
Concept: Seborrheic dermatitis (SD) is a chronic, relapsing, and usually mild form of dermatitis that occurs in infants and adults with predilection for the scalp and face. Etiology is not established but of fungi of the genusMalassezia may play a role [22]. The mildest and most common form of scalp SD is dandruff.
Clinical manifestations: there are two different forms [2] one in adults with predilection for the scalp, face, and intretriginous areas with well-demarcated, erythematous plaques with greasy-looking, yellowish scales distributed on areas rich in sebaceous glands (Fig9); and the lactant form with scaly and greasy lesions over an erythematous base in the diaper area, skin folds, centrofacial zone and the scalp where it can produce the craddle cap (Fig10).

Differential diagnosis: In children with atopic dermatitis and in adults with other erythematosquamous diseases as psoriasis.
Treatment: antifungal shampoos and creams containing mild corticosteroids or a combination of both are the main therapies [23-25]. Maintenance treatment in frequent relapsing cases should be considered. Prevention and how to control the progression of SD: there are no prevention strategies for this disease.
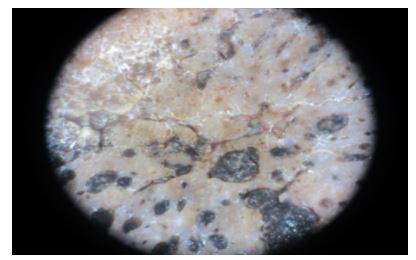
Concept: Seborrheic keratoses (SK) are common often multiple, epithelial tumours which usually appear in middle life consisting of a benign proliferation of immature keratinocytes.
Clinical manifestations: sharply demarcated gray-brown to black papules or plaques which are slightly raised and may be covered by greasy scales [2] (Fig11).
Differential diagnosis: Diagnosis usually based on the clinical appearance, but in pigmented lesions, or when the diagnosis would be uncertain or melanoma is suspected, a biopsy must be performed26. Examination with a dermatoscope may help (Fig 12).
Treatment: Is not necessary because they are benign lesions. Curettage with biopsy is recommended in doubtful lesions and electrodessication or cryotherapy are the more adequate techniques to eliminate SK. Cryotherapy is our preferred one.
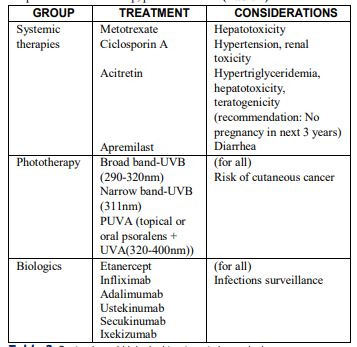
Concept: Psoriasis is a multisystemic inflammatory disease associated with a variety of comorbidities. It has a chronic course; unpredictable evolution and familiar aggregation and can begin at any age. The prevalence of psoriasis in adults ranged from 0.91 to 8.5 percent [27]. Psoriasis is a complex immune-mediated disease with genetic factors playing an important role.
Clinical manifestations: The major clinical categories include: chronic plaque psoriasis, guttate psoriasis, pustular psoriasis, erythrodermic psoriasis, inverse psoriasis, nail psoriasis. Chronic plaque psoriasis is the most common one, presenting with symmetrically distributed cutaneous erythematous scaly and well-demarcated plaques(Fig13), usually asymptomatic but sometimes pruriginous. The scalp, extensor elbows, knees, and gluteal cleft are the most common sites for involvement. Cardiovascular diseases, hypertension, metabolic syndrome, diabetes, neoplasms, inflammatory bowel disease and autoimmune disorders are more frequent in psoriatic patients than in general population [28-31].

Diagnosis and differential diagnosis: A diagnosis of psoriasis can be made by history and physical examination in the majority of cases, but in some cases a biopsy must be performed to rule out other skin diseases.
Treatment: Topical treatment with corticosteroids alone or in association with Vitamine D analogues may be useful in mild cases of psoriasis and the corticosteroid potency must be decided according to the anatomical site of involvement. Systemic therapies [33,34] are preferred for psoriasis affecting more than 10% of the body surface or more tan 5% in special sites as the scalp, palms and soles (Table 2)
Prevention and how to control the progression of psoriasis: some studies reveal that controlling metabolic syndrome psoriasis can improve.
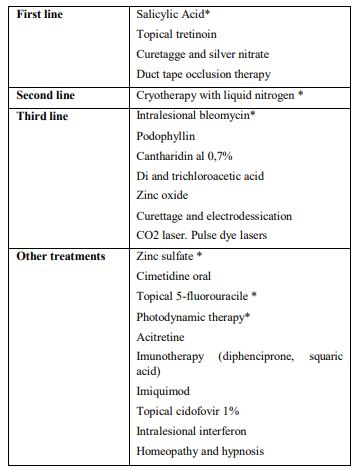
Concept: they are benign epithelial proliferations of the skin and mucous membranes caused by infection with one of many varieties of the human papillomavirus (HPV). Warts may be found in any location of the skin in persons of all ages.
Clinical presentation: the wart is the clinical expression of the HPV infection. They could be hyperkeratotic and exofitic papules or nodules, grey, yellowish or skin coloured (Fig14). Palms and soles are typical locations for viral warts, and in these 2 locations they use to have black dots corresponding to thrombosed capillaries.

Diagnosis and differential diagnosis: In typical lesions the clinician must not have diagnostic problems just with clinical examination, but sometimes a biopsy is required to differentiate them from seborrheic keratosis, lichenoid keratosis, amelanotic melanoma and others.
Treatment: Most of viral warts resolve spontaneously, so treatment must to be simple, little harmful and low cost with individual decision based on each patient. Available therapies are shown on table 3 [35-38].
Prevention and how to control the progression of warts: there are no prevention strategies to avoid viral warts and human papillomavirus contact.
Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.





























































